



Cystatin C: A Biomarker of Renal Dysfunction
Cystatin C (CysC) is an extraordinary protein known for its multifaceted functions. It serves as an early indicator for acute kidney injury (AKI), stands out as a superior gauge for both kidney transplant efficacy and the risk of transplant failure, and provides a more precise assessment of liver cirrhosis. Studies have indicated the potential of cystatin C in enhancing the diagnosis and prognosis of cardiovascular (CVD) risk as well as in oncology1.
Chronic Kidney Disease
Prevalence
Chronic kidney disease (CKD) represents a severe and progressive condition characterized by a gradual decline in kidney function. It poses a substantial global burden, affecting more than 10% of the world’s population, surpassing 800 million individuals, with a significant portion remaining undiagnosed. It impacts diverse demographic groups, including older adults, women, racial minorities, and individuals with hypertension or diabetes. Particularly in low- and middle-income countries, where resources for effective management are scarce, the burden of CKD is notably high2.
Over the past two decades, CKD has emerged as a leading cause of mortality worldwide, witnessing a rise in associated deaths. This trend has made it one of the foremost causes of death and suffering in the 21st century. Contributing to its prevalence is the increase in risk factors such as obesity and diabetes. While mortality rates among patients with end-stage kidney disease (ESKD) have shown a decrease, CKD continues to significantly impact global mortality, as indicated by the Global Burden of Disease (GBD) studies.
Addressing CKD requires urgent improvements in identification, monitoring, and treatment, alongside the implementation of preventive and therapeutic strategies on a global scale2.
Initiatives aimed at tackling CKD should not only focus on treatment but also emphasize prevention strategies, considering its link to modifiable risk factors like obesity and diabetes. Furthermore, there is a need for increased focus on comprehending CKD epidemiology across different demographics, including pediatric patients, and evaluating its implications on clinical outcomes like cardiovascular disease (CVD). By addressing these facets holistically, healthcare systems can effectively alleviate the negative repercussions of CKD and enhance patient outcomes on a global scale. 2.
Economic Burden
CKD poses a significant economic challenge on a global scale, particularly as it advances to kidney failure. The need for resource-intensive kidney replacement therapy (KRT), such as dialysis or kidney transplantation, imposes substantial healthcare expenses and societal burdens. Furthermore, as CKD progresses, there is an increased risk of cardiovascular disease (CVD), including heart failure, myocardial infarction, and stroke, which further amplifies healthcare resource utilization and economic strain. This dual impact, affecting both healthcare costs and societal burdens, underscores the critical importance of effective management and prevention strategies for CKD. Table 1 below illustrates the expenses associated with disease progression and severity, along with additional costs related to complications. 3.
| Table 1: Economic Burden of CKD & Associated Complications 3 | |
| Disease State / Intervention | Cost |
| Acute Kidney Injury (AKI) | $5,975 |
| Stage G3a | $3,060 |
| Haemodialysis | $57,334 |
| Peritoneal dialysis | $49,490 |
| Transplant | $75,326 |
| Myocardial infarction | $18,294 |
| Heart failure | $8,463 |
| Stroke | $10,168 |
Timely identification and intervention play a vital role in reducing the detrimental consequences of CKD. The implementation of early testing strategies, especially among high-risk groups such as individuals with diabetes, hypertension, and obesity, can facilitate the detection of CKD during its initial phases when interventions are most impactful 3.
CKD Classification
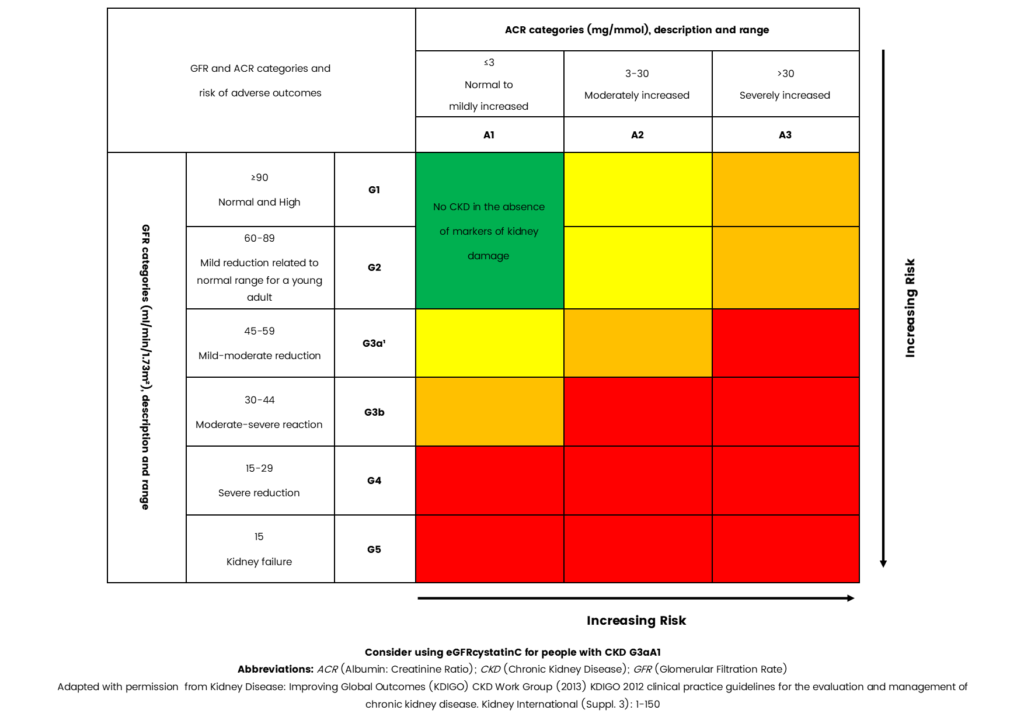
The contemporary categorization of CKD relies on a blend of estimated glomerular filtration rate (eGFR) and urinary albumin-to-creatinine ratio (ACR), as depicted in Figure4.
Elevated urinary albumin-to-creatinine ratio (ACR) and reduced glomerular filtration rate (GFR) are each linked independently to heightened risks of adverse events such as cardiovascular incidents (CVEs), kidney failure, and mortality. When both elevated ACR and decreased GFR coexist, the risk of adverse events is significantly amplified, signaling a more severe manifestation of kidney disease. This underscores the necessity of incorporating both markers into the evaluation and care of CKD patients4.
Figure 1: Classification of CKD using eGFR and urinary ACR categories 4
Cystatin C serves as an additional marker of kidney function that can enhance estimated glomerular filtration rate (eGFR), particularly in scenarios where eGFR based on serum creatinine may lack precision. Notably, Cystatin C is less susceptible to factors like muscle mass variations, which can influence serum creatinine levels. Consequently, Cystatin C might offer a more precise evaluation of renal function in certain populations, particularly those with borderline kidney function or individuals without indications of proteinuria.
The KDIGO CKD Work Group suggests considering supplementary tests like Cystatin C for confirmatory assessments in specific situations where eGFR derived from serum creatinine might be unreliable. However, it’s essential to recognize that Cystatin C isn’t as widely accessible in clinical settings as serum creatinine testing, and its utilization may hinge on local laboratory availability and practices4.
Aetiology of Cystatin C
Cystatin C, a 13kDa protein encoded by the CST3 gene, is a non-glycosylated, basic protein present in all nucleated cells. It acts as a potent inhibitor of lysosomal proteinases and extracellular inhibitors of cysteine proteases, thus playing a crucial role in regulating diverse cellular processes such as protein degradation, apoptosis (programmed cell death), and immune response modulation1.
A pivotal function of Cystatin C is its role in assessing renal function, particularly filtration. It is produced at a relatively constant rate and undergoes processes like filtration, reabsorption, and catabolism in the proximal tubule of the nephron. As Cystatin C remains unaffected by factors such as sex, age, or muscle mass, it is considered a more precise marker of renal function. Its minimal susceptibility to external influences compared to creatinine makes it widely regarded by healthcare professionals as a more dependable indicator for estimating glomerular filtration rate (GFR), the primary measure of renal function. Hence, Cystatin C measurements are frequently used alongside creatinine measurements to offer a more accurate evaluation of renal health1.
Furthermore, Cystatin C has been implicated in various other physiological processes and pathological conditions, including cardiovascular disease, neurodegenerative disorders, and cancer. This underscores its broader significance in human health beyond its role in assessing renal function1.
A Biomarker of Renal Dysfunction
Several studies support the utility of cystatin C as a biomarker of renal dysfunction.
- Cystatin C predicts long term mortality better than creatinine in a nationwide study of intensive care patients (2021) 5
A prospective study conducted in Sweden assessed 22,488 intensive care unit (ICU) patients across three hospitals in Sweden from 2004 to 2015, with a median follow-up period of 5.1 years. The study aimed to evaluate the predictive accuracy of estimated glomerular filtration rate (eGFR) using various equations based on creatinine, cystatin C, and a combination of both in critically ill patients.
The results indicated that employing a cystatin C-based equation for estimating GFR might offer superior risk prediction for mortality in critically ill patients compared to using creatinine-based equations. Consequently, the study advocates for the utilization of Cystatin C as a biomarker for eGFR in this specific patient population.
- Serum cystatin C as a biomarker for early diabetic kidney disease and dyslipidemia in young type 1 diabetic patients (2022) 6
A study conducted in Lithuania prospectively examined 779 participants, with a median age of 16.2 years and a median duration of diabetes of 5.3 years. The aim was to investigate the clinical relevance of serum cystatin C in the early identification of renal injury and its correlation with dyslipidemia among young individuals with type 1 diabetes (T1D).
The study’s results concluded that cystatin C can serve as an additional biomarker for the early detection of renal injury in young patients with T1D. Additionally, the findings suggest a connection between cystatin C levels and both glycemic control (HbA1c) and HDL cholesterol levels.
- Circulating cystatin C is an independent risk marker for cardiovascular outcomes, development of renal impairment, and long-term mortality in patients with stable coronary heart disease: The LIPID Study (2022) 7
A study conducted in the United States involving 7,863 patients, with a follow-up of 6,106 individuals from the LIPID (Long-Term Intervention with Pravastatin in Ischemic Disease) study, who had previously experienced acute coronary syndrome aimed to examine the correlation between circulating levels of cystatin C and various health outcomes in this specific patient cohort.
In summary, the study emphasizes Cystatin C as a strong and independent predictor of major cardiovascular events, the development of chronic kidney disease (CKD), as well as both cardiovascular and all-cause mortality among patients with stable coronary heart disease (CHD). Its predictive capability surpasses that of traditional markers of renal function, highlighting its importance in risk assessment and clinical management of individuals with CHD.
- Assessment of cystatin C level for risk stratification in adults with chronic kidney disease (2022) 8
A population-based cohort study conducted in the United Kingdom prospectively examined 428,402 patients recruited between 2006 and 2010, with a median follow-up period of 11.5 years. Participants were categorized into older (aged 65-73 years) and younger (<65 years) groups.
The study underscores the significance of evaluating renal function by measuring cystatin C levels alongside serum creatinine to achieve more precise risk stratification in individuals with mild chronic kidney disease (CKD). The integration of cystatin C assessment into clinical practice has the potential to improve the identification of individuals at heightened risk of cardiovascular disease (CVD) and mortality, thereby guiding clinical decision-making and enhancing patient outcomes.
Conclusion
In summary, unlike creatinine, cystatin C is less susceptible to influences from factors such as muscle mass, age, sex, and diet. This characteristic renders it particularly advantageous in populations where these variables may vary significantly, such as children, the elderly, and individuals with conditions characterized by muscle wasting. Moreover, Cystatin C has demonstrated its sensitivity as a marker for detecting early-stage renal dysfunction, often preceding changes in serum creatinine levels. Consequently, there is a growing trend in utilizing Cystatin C alongside creatinine to achieve a more precise assessment of renal function, especially in individuals affected by conditions like diabetes, chronic kidney disease (CKD), and cardiovascular disease (CVD). Overall, Cystatin C emerges as a valuable biomarker for estimated glomerular filtration rate (eGFR) and early detection of kidney dysfunction, providing clinicians with additional insights into a patient’s renal health beyond conventional markers like creatinine.
Fortress Cystatin C Solutions
| Description | Cat Code | Kit Size | Category |
| Cystatin C (L.S) Turbidimetric | BXC0777A | R1: 1 x 20ml R2: 1 x 4ml | Clinical Chemistry Reagent |
| Cystatin C | HIT0777A | R1: 2 x 20ml R2: 1 x 10ml | Analyser Specific Reagent |
| Cystatin C | BXCF777A | R1: 2 x 17.6ml R2: 2 x 6.1ml | Analyser Specific Reagent |
| Cystatin C Calibrator Set Level 1 – 6 | BXC0334A | 6 x 1ml | Calibrator & Controls |
| Cystatin C Control Level 1 | BXC0333A | 2 x 1ml | Calibrator & Controls |
| Cystatin C Control Level 2 | BXC0333B | 2 x 1ml | Calibrator & Controls |
Quote our promotional code ‘CYSC24’ for a discount on Cystatin C products.
References
- Fernando S, Polkinghorne KR. Cystatin C: not just a marker of kidney function. Brazilian Journal of Nephrology 2020; 42(1). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7213924/ (accessed 14 February 2024).
- Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney International Supplements 2022; 12(1). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9073222/ (accessed 14 February 2024).
- Jha V, Al-Ghamdi SMG, Li G, Wu MS, Stafylas P, et al. Global Economic Burden Associated with Chronic Kidney Disease: A Pragmatic Review of Medical Costs for the Inside CKD Research Programme. Advances in Therapy 2023; 40. https://link.springer.com/article/10.1007/s12325-023-02608-9 (accessed 27 February 2024).
- National Institute of Care Excellence. What initial investigations should I arrange?. https://cks.nice.org.uk/topics/chronic-kidney-disease/diagnosis/initial-investigations/ (accessed 27 February 2024).
- Helmersson-Karlqvist J, Lipcsey M, Ärnlöv J, Bell M, Ravn B, et al. Cystatin C predicts long term mortality better than creatinine in a nationwide study of intensive care patients. Scientific Reports 2021; 11(5882). https://www.nature.com/articles/s41598-021-85370-8 (accessed 28 February 2024).
- Stankute I, Radzevičienė L, Monstaviciene A, Dobrovolskiene R, Danyte E, et al. Serum Cystatin C as a Biomarker for Early Diabetic Kidney Disease and Dyslipidemia in Young Type 1 Diabetes Patients. Medicina 2022; 58(2). https://www.mdpi.com/1648-9144/58/2/218 (accessed 28 February 2024).
- West M, Kirby A, Stewart RA, Blankenberg S, Sullivan D, et al. Circulating Cystatin C Is an Independent Risk Marker for Cardiovascular Outcomes, Development of Renal Impairment, and Long‐Term Mortality in Patients With Stable Coronary Heart Disease: The LIPID Study. Journal of the American Heart Association (JAMA) 2022; 11(5). https://www.ahajournals.org/doi/10.1161/JAHA.121.020745 (accessed 27 February 2024).
- Lees JS, Rutherford E, Stevens KI, Chen DC, Scherzer R, et al. Assessment of Cystatin C Level for Risk Stratification in Adults With Chronic Kidney Disease. Journal of the American Medical Association https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2797627 (accessed 28 February 2024).